A Clinician's Guide to Understanding the wRVU Compensation Model
Master the wRVU system. Learn how your work translates to compensation, how to negotiate your contract, and use wRVU knowledge to build a sustainable career.
A Relative Value Unit (RVU) is Medicare's way of assigning a point value to every service a physician provides. The work Relative Value Unit (wRVU) is a key component of this system. Think of it like a currency for clinical work. The more complex, intense, or time-consuming a service is, the more wRVU points it’s worth—and those points directly translate into your paycheck.
Deconstructing the wRVU and How It Impacts Your Paycheck
If you’ve ever stared at a physician employment contract, you've probably seen the acronym wRVU, which stands for Work Relative Value Unit. This one metric is often the engine driving your entire compensation plan, but it's a huge source of confusion for many clinicians.
Simply put, the wRVU isolates and quantifies your direct work in a patient encounter—the time, the mental effort, the technical skill, and the stress involved.
Let’s take a real-world example. An internist sees an established patient for a routine follow-up (CPT 99213) and later admits a complex new patient to the hospital (CPT 99223). The hospital admission takes far more time, clinical intensity, and decision-making. The wRVU system recognizes this by assigning a much higher point value to that admission, making sure the physician is paid proportionally for the more demanding work.
This is how the system separates what you do from the hospital’s own costs. But the wRVU is just one piece of a bigger puzzle.
The Three Components of a Total RVU
The total RVU for any given service is actually the sum of three different parts. Each one accounts for a different cost associated with providing medical care. Breaking them down is the key to understanding how your wRVU is valued from a financial perspective.
| RVU Component | What It Measures | Average Contribution to Total RVU |
|---|---|---|
| Work RVU (wRVU) | The physician's time, skill, intensity, and mental effort. This is the part that reflects your direct labor. | ~51% |
| Practice Expense RVU (PE RVU) | The overhead costs of running a practice—rent, equipment, supplies, and non-physician staff salaries. | ~45% |
| Malpractice RVU (MP RVU) | The cost of professional liability insurance premiums for a given specialty and service. | ~4% |
By pulling the physician’s work (wRVU) out from the practice and insurance costs, healthcare organizations get a clean, standardized way to measure individual productivity. It lets them make "apples-to-apples" comparisons of clinical output, no matter the practice setting.
While all three components are needed to calculate the final Medicare reimbursement for a service, your employment contract will almost always focus exclusively on the wRVU.
That's because it's the most direct measure of your clinical effort and productivity. After all, knowing your compensation structure is a crucial part of a physician's financial health. Getting a handle on your numbers is the first step to proactively managing your practice's finances and learning to care for your income. Mastering this metric is foundational to building a career that is not only financially sustainable but personally fulfilling.
To really get why the wRVU system exists—and why it’s a relatively fair way to measure physician work—you have to understand the mess it replaced. Before 1992, physician payment was the Wild West. Billing was governed by a vague, inconsistent system that left clinicians and payers guessing.
This old model was called the "Customary, prevailing, and Reasonable" (CPR) charge system. On paper, it sounded simple: Medicare would pay doctors based on what they and their local peers usually charged for a service.
In reality, CPR was a disaster. It had no objective standard for what a medical service was actually worth. Reimbursement was tied directly to a doctor’s own billing history. The result? Physicians who charged more got paid more, regardless of how complex the work was or how many resources it took.
The Problems with the Old CPR System
This charge-based model completely warped the healthcare market. It rewarded high billing, not efficient care, which sent costs spiraling and made payments unpredictable. The system was especially brutal for primary care physicians, as it heavily favored procedural specialists while devaluing crucial cognitive work.
The fallout was predictable:
- Massive Payment Disparities: Two doctors in the same city could get paid wildly different amounts for the exact same procedure.
- Financial Instability: With no standard value for services, trying to predict revenue was a nightmare for private practices and for Medicare itself.
- Perverse Incentives: The whole system encouraged doctors to just keep raising their fees, feeding unchecked healthcare inflation.
Under the CPR system, primary care was constantly getting squeezed. Reimbursement just didn't keep up with the growing complexity of patient management. Meanwhile, specialists performing procedures could inflate their charges much more easily, widening the income gap and sending a clear message that cognitive work was less valuable.
A New, Resource-Based Approach
By the late 1980s, everyone knew the CPR system was broken and unsustainable. Medicare was drowning in skyrocketing costs from a system that sometimes paid claims based on fees in the 90th percentile for a region. Something had to change.
The Centers for Medicare & Medicaid Services (CMS) teamed up with a Harvard research group to build a more logical framework. This effort led to the creation of the Resource-Based Relative Value Scale (RBRVS), which Congress officially authorized in 1989. For a deeper dive, you can learn more about how the RVU system was developed to help practices.
This was a total paradigm shift. Instead of basing payments on historical charges, the RBRVS assigned value to a service based on the actual resources needed to perform it. This included the physician’s work, practice overhead, and malpractice insurance costs.
On January 1, 1992, this new model was rolled out in the Medicare Physician Fee Schedule. This was the birth of the RVU system as we know it today—designed to bring objectivity, predictability, and a bit more fairness to how physicians get paid. It laid the foundation for the wRVU-based contracts that have become the standard across medicine.
How Your wRVU Value Translates into Dollars
So you’ve put in the work and racked up the wRVUs. That's great, but how do those points actually turn into money in your bank account? It’s not magic; there's a specific formula that connects your clinical effort to your paycheck.
Think of it like a recipe. Your wRVU is the main ingredient, but two other key multipliers—the GPCI and the Conversion Factor—are needed to get the final dollar amount.
First, a little context helps. The RVU system didn't just appear out of nowhere. It was designed to bring order to a chaotic physician payment landscape.
This flowchart shows how we got from the old, inconsistent CPR system to the standardized, resource-based model we use today.
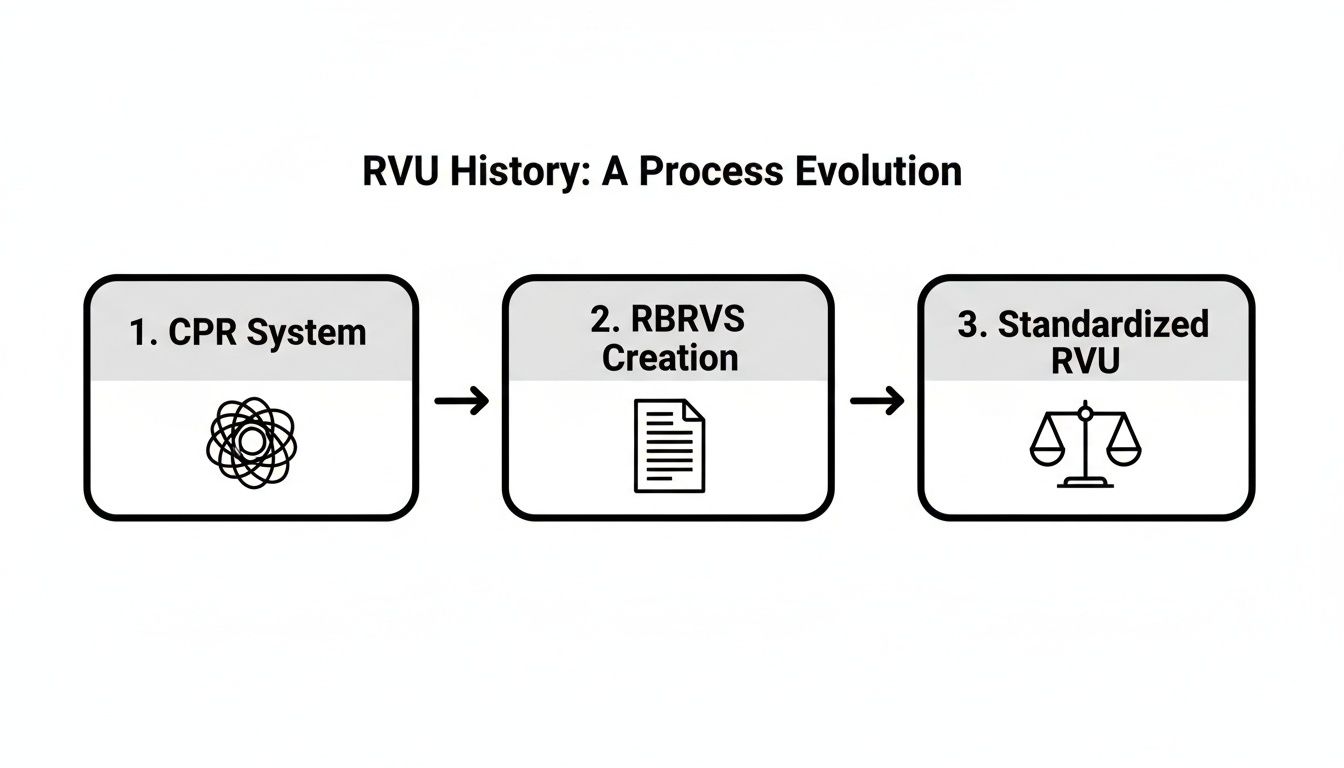
This shift was a deliberate move toward a more objective and fair way to value physician work, and understanding the steps is key to mastering your compensation.
Step 1: Start with the Total RVU
While your employment contract probably zeroes in on your work RVUs (wRVUs), the full Medicare reimbursement formula actually starts with the Total RVU. This figure is simply the sum of all three RVU components:
- Work RVU (wRVU): Your direct clinical effort.
- Practice Expense RVU (PE RVU): The overhead costs of running the practice.
- Malpractice RVU (MP RVU): The cost of professional liability insurance.
Each medical service has a value assigned to these three parts, and adding them together gives you the complete value for that service before any other adjustments are made.
Step 2: Apply the Geographic Adjustment
Next up, the system has to account for the fact that it costs more to run a practice in downtown San Francisco than in rural Kansas. This is where the Geographic Practice Cost Index (GPCI) comes in.
The GPCI isn't just one number; it’s a set of three different adjusters that are applied to each part of the Total RVU:
- Work GPCI: Adjusts for local differences in physician labor costs.
- Practice Expense GPCI: Adjusts for regional variations in rent, staff salaries, and supplies.
- Malpractice GPCI: Adjusts for the local cost of malpractice insurance premiums.
You multiply each RVU component by its corresponding GPCI adjuster. Adding those three numbers together gives you the Geographically Adjusted Total RVU. This crucial step ensures the final payment reflects the real-world cost of providing care in a specific city or region.
The formula breaks down like this: (wRVU x Work GPCI) + (PE RVU x PE GPCI) + (MP RVU x MP GPCI) = Geographically Adjusted Total RVU
Step 3: Use the Conversion Factor to Get Your Final Payment
This is the final and most straightforward step. The Conversion Factor (CF) is a single, national dollar amount that CMS sets each year. It’s the master multiplier that converts your geographically adjusted RVU total into a concrete dollar figure.
For 2024, the Medicare Conversion Factor is $32.74.
To find the final Medicare reimbursement for a service, you just multiply the Geographically Adjusted Total RVU by this year's Conversion Factor. The result is the total amount Medicare will pay for that CPT code.
This fundamental math is the foundation for most wRVU-based physician compensation models. If you want to see how different wRVU targets or conversion factors could impact your take-home pay, you can run the numbers using our Salary & FIRE Calculator. It's built to help you model out these scenarios and plan your financial future with more clarity.
Decoding Your wRVU Compensation Structure
Knowing the theory behind the wRVU is one thing, but understanding how they show up in your employment contract is what really matters. Employers use wRVUs to build all sorts of compensation plans, and each one comes with its own set of incentives and risks. Getting a handle on these models is critical before you sign on the dotted line.
The shift to wRVU-based pay has been massive. Today, around 70% of physician contracts in the U.S. use wRVUs to determine at least part of a clinician's pay. In these setups, productivity often drives 40-60% of your total compensation, usually through a base salary paired with bonuses for hitting specific targets, like generating 10,000 wRVUs in a year.
The wRVU component itself, which isolates your direct clinical work, makes up about 52% of a service's total RVU value. For instance, a basic office visit (CPT 99213) is worth roughly 1.3 wRVUs, while a more involved procedure like a colonoscopy might be valued around 3.5 wRVUs. When you multiply these points by the annual Medicare conversion factor—$32.74 in 2024—and any local geographic adjustments, they become the reimbursement dollars that ultimately fund your salary. For a deeper dive, you can learn more about how RVUs are used in provider compensation across the industry.
To give you a better idea of how these values compare, here’s a quick look at some common services across different specialties.
Sample wRVU Values for Common Medical Services
This table shows the approximate work RVU values for a few common CPT codes. It’s a great way to see how different clinical activities are valued relative to one another.
| Specialty | CPT Code | Service Description | Approximate wRVU Value |
|---|---|---|---|
| Family Medicine | 99213 | Established patient office visit, low complexity | 1.30 |
| Internal Medicine | 99214 | Established patient office visit, mod. complexity | 1.92 |
| Cardiology | 93000 | Standard 12-lead EKG with interpretation | 0.25 |
| Dermatology | 17000 | Destruction of premalignant lesion, first lesion | 0.65 |
| General Surgery | 47562 | Laparoscopic cholecystectomy | 12.87 |
| Orthopedics | 27447 | Total knee arthroplasty | 22.50 |
| Gastroenterology | 45378 | Diagnostic colonoscopy | 3.53 |
| Emergency Medicine | 99284 | ED visit, high complexity, urgent problem | 2.60 |
| Psychiatry | 90837 | Psychotherapy, 60 minutes | 2.37 |
| Obstetrics/Gynecology | 59400 | Routine obstetric care including delivery | 34.25 |
Keep in mind these are just approximations. The actual values can shift based on updates from CMS and other factors, but they illustrate the basic principle: more complex and time-consuming work is assigned a higher wRVU value.
Now, let's break down the most common compensation models you'll run into.
Common wRVU Compensation Models
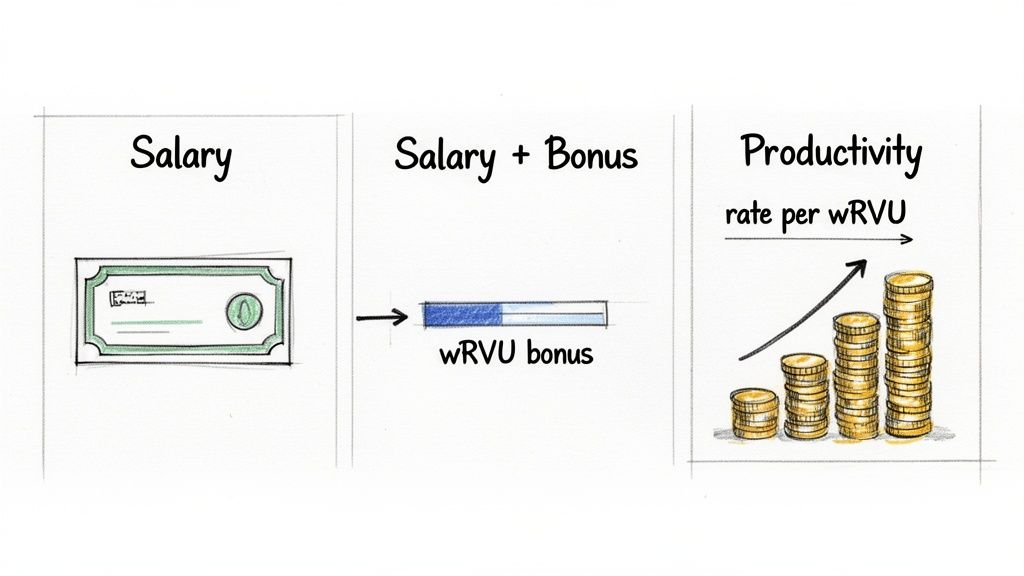
While contracts can get creative, most will fall into one of three main buckets. Each model strikes a different balance between the security of a guaranteed salary and the financial upside of being highly productive. Figuring out which one fits your work style and financial goals is key.
Straight Salary with a wRVU Target: With this model, you get a fixed annual salary as long as you meet a minimum wRVU threshold. For example, a pediatrician might be offered $200,000 per year with a target of hitting 4,500 wRVUs. It’s predictable, but there’s often no direct financial reward for blowing past your target.
Base Salary Plus a Productivity Bonus: This is probably the most common hybrid model out there. It gives you the stability of a base salary plus a bonus for every wRVU you generate above a set threshold. A hospitalist, for instance, might have a $250,000 base salary and earn a bonus for every wRVU over 4,800 for the year.
Straight Production (100% wRVU-Based): This is the high-risk, high-reward option. Your entire income is calculated by multiplying your total wRVUs by a negotiated dollar amount, known as the rate per wRVU. If an orthopedic surgeon has a rate of $50 per wRVU and generates 9,000 wRVUs, their gross income is $450,000. Simple as that.
The "rate per wRVU" is one of the most critical negotiation points in any productivity-based contract. This single dollar amount can vary dramatically based on your specialty, geographic location, and the negotiating power of the health system.
A Real-World Bonus Calculation Example
Let's make this concrete. Imagine you're an internal medicine physician looking at a job with a hybrid compensation plan.
- Base Salary: $220,000 per year.
- wRVU Threshold: 4,200 wRVUs annually.
- Bonus Rate: $45 for every wRVU generated above the threshold.
Let's say you have a busy year and generate a total of 5,000 wRVUs. The bonus math is pretty simple. First, you figure out how many wRVUs you produced over your target: 5,000 (total) - 4,200 (threshold) = 800 wRVUs.
Next, you multiply that surplus by your bonus rate: 800 wRVUs x $45/wRVU = $36,000.
Your total compensation for the year would be your base salary plus that bonus: $220,000 + $36,000 = $256,000. This is exactly how your clinical effort translates into cash in your bank account, and it empowers you to look at any job offer and know exactly how your work will be valued.
Using wRVU Knowledge to Prevent Burnout
The constant demand to generate wRVUs can feel like a productivity treadmill with no off-switch. This relentless focus on volume is a huge driver of physician burnout, turning medicine into a numbers game.
But what if you could use the system to your advantage? A deep understanding of how the wRVU works is one of the most powerful tools you have for designing a sustainable career. It’s not about working harder—it’s about working smarter.
Instead of letting the wRVU model dictate your schedule and your life, you can use it as a strategic map. It can guide you toward a career that's both financially rewarding and personally sustainable, putting you back in control.
Shifting from Volume to Value
The core issue with most wRVU compensation models is the built-in incentive to see as many patients as possible. This high-volume approach inevitably leads to shorter appointments, more administrative work, and feeling like a cog in a machine. That’s the fast track to exhaustion.
The smarter alternative is to focus on higher-value work. By analyzing the wRVU values for different CPT codes in your specialty, you can find opportunities to meet your income targets in fewer hours. This could mean developing a niche skill or focusing on more complex cases that carry a higher wRVU weight.
For example, a family medicine physician might find that performing in-office procedures generates far more wRVUs per hour than routine office visits. By strategically scheduling these procedures, they can hit their productivity goals more efficiently, freeing up time for other passions—or just for a break.
The Rise of Burnout-Friendly Roles
The structure of your job plays a massive role in how wRVU pressure affects you. A traditional hospital job with a heavy call burden and weekend shifts only magnifies the strain. Fortunately, new models are emerging that better align financial stability with work-life balance.
- Telehealth Opportunities: Remote care has created new ways to generate wRVUs without the physical and emotional drain of being in a clinic all day. These roles often eliminate commutes and cut down on administrative tasks, letting you focus on patient care.
- No-Call, Weekday-Only Positions: More and more employers are finally recognizing the need for sustainable careers. Roles without call responsibilities or weekend shifts are becoming more common, designed specifically to prevent the burnout that comes with a 24/7 work culture.
For clinicians feeling the strain, the wRVU system can highlight common traps. An over-reliance on high-volume wRVU chasing is a major cause of exhaustion. Some studies show that physicians who generate over 12,000 wRVUs a year report 40% higher burnout rates.
In contrast, a curated no-call telehealth job might average around 5,500 wRVUs with weekends completely free—a model that works for long-term financial and personal goals. For instance, a $250,000 salary from 6,000 wRVUs can fund retirement in just 12 years with a 7% market return. Similarly, psychologists billing for 45-minute therapy sessions (CPT 90834, 1.85 wRVUs) can thrive in remote settings, hitting 4,000 units annually without the overhead of a physical office. You can learn more about how relative value units are structured on aapc.com.
Understanding your personal burnout risk is the first step toward building a better career. By identifying the specific workplace stressors that affect you most, you can begin to make targeted changes that protect your long-term well-being.
Taking Control of Your Career Path
The ultimate message here is one of empowerment. Stop letting the wRVU system use you. Instead, see it as a tool—a set of rules you can learn and master for your own benefit. When you combine your clinical expertise with a solid grasp of compensation mechanics, you can actively shape a career that supports your financial goals without costing you your health.
This strategic approach helps you step off the productivity treadmill and build a professional life that’s both profitable and personally fulfilling. If you're wondering how your current role stacks up, our platform has tools to help you assess your situation. You might be interested in calculating your personal burnout score to get a clearer picture.
How to Negotiate Your wRVU Contract with Confidence
Once you have a firm grip on the wRVU system, you can stop being a passive recipient of a job offer and start being an active architect of your career. Negotiation isn't about being confrontational. It's about making sure your compensation truly reflects the value you bring to the table. The trick is knowing which levers to pull.
When you're looking at a wRVU-based contract, your negotiation should laser-focus on four key components. Each one has a direct line to your earning potential and your work-life balance, so getting them right from the start is absolutely crucial.
Pinpoint Your Key Negotiation Levers
Before you even think about putting pen to paper, you need total clarity on these four points. They are the engine of your compensation plan and the biggest opportunities you have to shape your contract for the better.
- The Base Salary: This is your financial floor, your safety net. Make sure it’s competitive for your specialty and location by checking benchmark data from places like the Medical Group Management Association (MGMA). A solid base salary takes the pressure off, so you don't feel like you're in a mad dash to generate wRVUs from day one.
- The wRVU Productivity Threshold: This is the magic number—the total wRVUs you need to hit before you start earning a bonus. A lower threshold is your friend; it means you get to that bonus pay much sooner. You should ask how they came up with that target and if it accounts for the natural ramp-up time in a new role.
- The Bonus Rate Per wRVU: This is the dollar amount you’ll get for every single wRVU you generate above that threshold. This rate is almost always negotiable and can vary wildly between employers. A higher rate is a direct reward for your efficiency and hard work.
- Credit for Non-Clinical Work: This is a big one. Will you get wRVU credit for the time you spend on administrative tasks, teaching residents, or doing research? Getting these activities written into your contract is a huge win. It shows that your employer values your entire contribution, not just the clinical grind.
Knowing your numbers is only half the battle. Truly mastering the real principles of negotiating can completely change the game, leading to better terms and a much better final offer. It's about doing your homework, understanding what the other side needs, and clearly communicating your value.
Questions to Ask Your Potential Employer
A great negotiation is built on information. Asking smart, targeted questions doesn't just show you've done your research—it helps you uncover potential red flags and hidden opportunities.
Don't just accept the numbers on the page. A truly good offer includes the operational support needed to help you succeed. An amazing bonus structure is worthless if clinic inefficiency prevents you from ever hitting your targets.
Walk into that negotiation with a checklist of questions. This ensures there are no nasty surprises waiting for you down the road.
- How is wRVU credit split for procedures or services shared with Advanced Practice Providers (APPs)?
- What's the process for auditing and reconciling wRVU reports? How often does that happen?
- What specific operational support is in place to help me work efficiently? Think scribes, a user-friendly EMR, or quick room turnover.
- How are wRVU targets and bonus rates adjusted year over year? What factors influence those changes?
When you ask these questions, the entire conversation shifts. You're no longer just talking about a salary; you're co-designing a job that sets you up for success and prevents burnout in the long run. If you want to dig deeper into an offer, using an offer analyzer tool for clinicians can be incredibly helpful.
At WeekdayDoc, we believe that understanding your compensation is the first step toward building a sustainable career. Our platform is dedicated to helping clinicians find burnout-friendly roles that respect your time and value your expertise. Explore curated no-call, weekday-only jobs at https://www.weekdaydoc.com.